VA Disability Ratings for Anxiety

CCK Law: Our Vital Role in Veterans Law
In one 2024 study, about 7.9 percent of veterans screened positive for Generalized Anxiety Disorder (GAD), while 22.1 percent showed symptoms of mild anxiety. These rates of anxiety are significantly higher than the civilian population, of which only 2.7 percent are diagnosed with GAD.
If you are a veteran suffering from anxiety due to your service, this article will guide you through the essentials of VA’s disability claims process so you can earn an anxiety VA rating and compensation.
Key takeaways:
- Veterans can earn anxiety disability ratings of 0, 10, 30, 50, 70, or 100 percent from the Department of Veterans Affairs (VA).
- Though in-service records and medical treatment records are important for veterans to establish service connection for their anxiety, lay statements can also contribute substantially by filling gaps in a veteran’s body of evidence.
- It is possible to earn total disability for anxiety, either through a 100 percent schedular rating, or through Total Disability based on Individual Unemployability (TDIU), which is available to eligible veterans whose anxiety prevents them from maintaining gainful employment.
Who We Are: Chisholm Chisholm & Kilpatrick (CCK Law) has argued many of the cases that define and clarify veterans disability law. Our attorneys serve in many leadership positions and have posted more than 2,500 blogs and 1,100 videos explaining veterans benefits. With 100+ individuals accredited by VA or admitted to practice before the U.S. Court of Appeals for Veterans Claims, CCK Law has recovered over $1 billion in compensation for 36,000+ clients since 1999. (Past results do not guarantee future outcomes.) Contact us to tell us about your case.
What Is Anxiety?
Anxiety is defined as intense, excessive, and persistent worry and fear about everyday situations. The most common symptoms of anxiety disorders include the following:
- Feeling restless, jumpy, or on edge,
- Excessive worrying,
- Difficulty concentrating,
- Rapid heartbeat,
- Trembling or twitching,
- Muscle tension,
- Shortness of breath or difficulty breathing,
- Feeling dizzy, nauseous, or lightheaded, and
- Difficulty sleeping.
There are several types of anxiety disorders, such as generalized anxiety disorder, panic disorder, and various phobia-related disorders. Veterans suffering from anxiety disorders may be eligible for VA disability benefits if they can demonstrate that their anxiety is due to their military service.
For more information on how to win VA anxiety claims, watch this video from Kayla Rogers and Bethany Cooke, VA-accredited claims advocates at CCK Law:
How Do I Prove Service Connection for Anxiety Disorders?
One of the first steps to earning a VA disability rating for anxiety is for veterans to prove that their anxiety is somehow related to their military service. This is called establishing service connection, and there are several ways to do so, such as directly, secondarily, or through aggravation.
Direct Service Connection for Anxiety
Direct service connection is when a veteran can prove that their military service either directly caused or worsened their anxiety. To establish direct service connection for an anxiety disorder, veterans must establish the following:
- A current diagnosis of an anxiety disorder;
- An in-service occurrence that caused or aggravated the anxiety disorder; and
- A medical nexus (e.g., professional medical opinion) connecting the current, diagnosed anxiety disorder to the in-service occurrence.
Examples of in-service occurrences might include if a veteran is specifically treated for their anxiety during their time in service, or if they check off that they are experiencing anxiety-like symptoms at the time of their discharge examination.
It is important to note that the in-service occurrence element of service connection does not require that the veteran have an official diagnosis of an anxiety disorder during service.
Instead, a veteran can be diagnosed with an anxiety disorder following service and still receive benefits if they can establish their current condition is connected to service. A medical opinion is almost always required to establish this nexus.
Secondary Service Connection for Anxiety
Secondary service connection represents an alternative way to get service connection for anxiety. In this case, if veterans have an already service-connected condition that is either causing or aggravating their anxiety, then secondary service connection may be warranted.
For example:
- Say a veteran has a service-connected knee condition that causes significant pain and impedes their ability to carry out everyday activities and tasks.
- After years of dealing with their limited mobility, the veteran becomes very anxious about their functionality and ability to live a normal life. The veteran’s doctor notices this newfound anxiety and offers the veteran their opinion that the veteran’s knee condition may be the root cause for its development.
- Here, the veteran may be entitled to secondary service connection for their anxiety, since it was brought on as a result of their service-connected knee condition.
What if Veterans Were Diagnosed With Anxiety Before Service?
Even if a veteran received an initial diagnosis of an anxiety disorder before entering the military, they may still qualify for VA disability benefits.
In this case, the veteran would need to prove that his or her military service aggravated, or worsened, the preexisting anxiety disorder beyond its natural progression. This is called service connection based on aggravation.
For example:
- Say a new servicemember suffers from mild anxiety before joining the military, for which a doctor officially diagnoses them.
- During the service member’s military service, the stress of being deployed overseas takes its toll on their mental health, and their anxiety worsens substantially, beyond the normal course of progression. This is proven by several in-service medical records where it is mentioned that the service member is now suffering panic attacks.
- If the service member’s anxiety persists at this level of severity even after they leave the military, then they may be entitled to service connection based on aggravation, since their time in the service worsened their anxiety more than if they had not joined.
What Evidence Do I Need To Provide for My Anxiety Claim?
There are multiple kinds of evidence a veteran can submit to prove their anxiety claim to VA. Some of these include:
- In-Service Records – Records from a veteran’s time in the military are one of the most important pieces of evidence they can submit to VA to prove their claim. Examples include a medical report where the veteran expresses newfound feelings of anxiety, or an incident report where the veteran suffers from a panic attack.
- Medical Records and Opinions – Medical records or opinions from a veteran’s doctor will also serve their case well. For instance, if the veteran’s physician gives their opinion that a trauma the veteran experienced in service likely led to them developing anxiety, this would serve as a nexus.
- Another form of evidence that veterans could use for their anxiety claim is lay evidence, which are accounts from a veteran or their friends, family, or fellow service members that describe the veteran’s symptoms.
“Lay evidence is one of the things we go to most often for anxiety claims,” says Nicholas Briggs, VA-accredited claims advocate with CCK Law. “This is largely because veterans don’t often feel comfortable seeking treatment for their anxiety during service or afterward, since it’s kind of stigmatized. Therefore, lay evidence from the veteran and their family members can help fill in gaps in the medical records.”
Compensation & Pension (C&P) Exams for Anxiety
Compensation & Pension (C&P) exams are medical examinations generally used by VA to determine if there is a nexus between the veteran’s current, diagnosed condition and their time in service. They are also used to evaluate the severity of a veteran’s symptoms to determine a disability percentage rating.
A C&P exam for anxiety might look like:
- Ahead of time, the VA examiner will likely review the veteran’s claim file to prepare for the examination.
- During the exam, the veteran will meet with their VA examiner, who will ask them questions about their medical history, time in service, and current condition.
- Next, the VA examiner might ask about the veteran’s current symptomatology to determine the severity of their anxiety disorder. This may include questions about how the veteran’s anxiety impacts their life on a day-to-day basis.
- Throughout the exam, the VA examiner will fill out a Disability Benefits Questionnaire, or DBQ. The DBQ is a form that helps the examiner collect information on the veteran’s specific anxiety symptoms and severity. Ahead of time, the veteran could also request their private doctor submit a DBQ to VA, which may help to hasten the claims process.
- After the exam, the VA examiner will write up a report to deliver to VA. This report will offer the examiner’s opinion on whether the veteran’s condition is service connected and how severe it is, for the purpose of assigning a disability rating.
If the VA examiner’s report ends up being unfavorable to the veteran’s claim, it is possible VA will deny that claim. To help mitigate this possibility, CCK Law’s Nicholas Briggs recommends the following:
“First and foremost, veterans need to make sure they’re requesting a copy of their VA examination, which they’re entitled to do,” says Briggs. “Once they have the exam, they should go through it at length making sure to identify any specific problems they noticed or things they think conflict with other evidence they’ve submitted before.”
After this, the veteran should follow up with VA to point out these discrepancies, which can be done by submitting additional evidence or argument.
Importantly, veterans should always attend their C&P exams or notify VA immediately if they cannot. Failure to attend a C&P exam will likely result in VA denying benefits.
How Does VA Rate Anxiety Disorders?
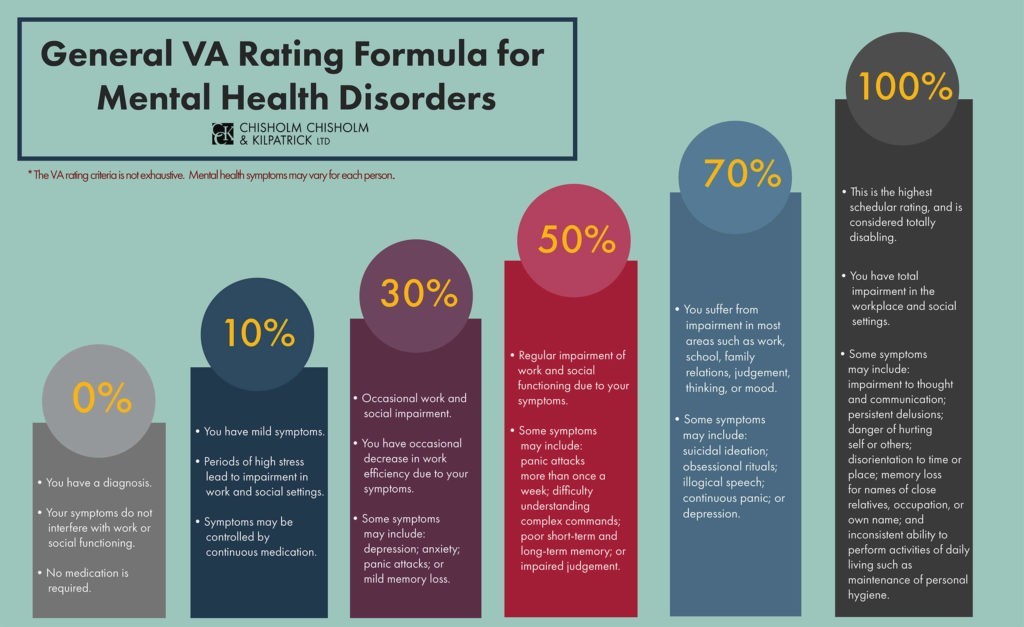
When rating service-connected anxiety disorders, VA uses the General Rating Formula for Mental Disorders included in 38 CFR § 4.130 to assign one of the following percentages: 0, 10, 30, 50, 70, or 100.
These ratings are based on the level of social and occupational impairment a veteran experiences and the severity of symptoms VA uses to characterize that impairment. The criteria for this formula are as follows:
- 100 percent – Total occupational and social impairment, due to such symptoms as: gross impairment in thought processes or communication; persistent delusions or hallucinations; grossly inappropriate behavior; persistent danger of hurting self or others; intermittent inability to perform activities of daily living (including maintenance of minimal personal hygiene); disorientation to time or place; memory loss for names of close relatives, own occupation, or own name.
- 70 percent – Occupational and social impairment, with deficiencies in most areas, such as work, school, family relations, judgment, thinking, or mood, due to such symptoms as: suicidal ideation; obsessional rituals which interfere with routine activities; speech intermittently illogical, obscure, or irrelevant; near-continuous panic or depression affecting the ability to function independently, appropriately and effectively; impaired impulse control (such as unprovoked irritability with periods of violence); spatial disorientation; neglect of personal appearance and hygiene; difficulty in adapting to stressful circumstances (including work or a work-like setting); inability to establish and maintain effective relationships.
- 50 percent – Occupational and social impairment with reduced reliability and productivity due to such symptoms as: flattened affect; circumstantial, circumlocutory, or stereotyped speech; panic attacks more than once a week; difficulty in understanding complex commands; impairment of short- and long-term memory (e.g., retention of only highly learned material, forgetting to complete tasks); impaired judgment; impaired abstract thinking; disturbances of motivation and mood; difficulty in establishing and maintaining effective work and social relationships.
- 30 percent – Occupational and social impairment with occasional decrease in work efficiency and intermittent periods of inability to perform occupational tasks (although generally functioning satisfactorily, with routine behavior, self-care, and conversation normal), due to such symptoms as: depressed mood, anxiety, suspiciousness, panic attacks (weekly or less often), chronic sleep impairment, mild memory loss (such as forgetting names, directions, recent events).
- 10 percent – Occupational and social impairment due to mild or transient symptoms which decrease work efficiency and ability to perform occupational tasks only during periods of significant stress, or symptoms controlled by continuous medication.
- 0 percent – A mental condition has been formally diagnosed, but symptoms are not severe enough either to interfere with occupational and social functioning or to require continuous medication.
All the following anxiety disorders are categorized by a diagnostic code (DC) and rated based on this general formula:
- DC 9400: Generalized anxiety disorder
- DC 9403: All phobias, including social anxiety disorder
- DC 9404: Obsessive-compulsive disorder
- DC 9410: Other specified anxiety disorder
- DC 9411: Post-traumatic stress disorder
- DC 9412: Panic disorder and/or agoraphobia
This portion of the rating schedule is based on the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). According to 38 CFR § 4.125, Diagnosis of Mental Disorders, if the diagnosis of a mental disorder does not conform to DSM-5, the rating agency will return the VA examination report to the examiner to substantiate the diagnosis.
Additionally, if the diagnosis of a mental disorder is changed, the rating agency will determine whether the new diagnosis represents:
- Progression of the prior diagnosis,
- Correction of an error in the prior diagnosis, or
- Development of a new and separate condition.
What Is the Difference Between a 50 Percent and a 70 Percent Anxiety Rating?
The criteria for 50 percent and 70 percent anxiety disability ratings are similar in terms of the language that is used when referencing occupational and social impairment:
- “50 percent – occupational and social impairment with reduced reliability and productivity…”
- “70 percent – occupational and social impairment, with deficiencies in most areas…”
VA has not yet provided exact definitions for the abovementioned phrases. However, the diagnostic codes provide examples of the types of symptoms that may fall under each. For example, in the 50 percent criteria, “reduced reliability and productivity” may include impaired judgment, impaired abstract thinking, panic attacks more than once per week, flattened affect, etc.
For the 70 percent rating criteria, “deficiencies in most areas” involve more aspects of life and may include suicidal ideation, obsessive rituals, and an inability to establish and maintain effective relationships.
In denying a higher disability rating for anxiety, VA must explain to veterans why they are not entitled to the higher rating by providing adequate reasons and bases. If VA fails to do so, then veterans have the right to appeal.
For further discussion of getting a 70 percent VA rating for mental health, check out this video with Kayla Rogers, VA-accredited claims agent with CCK Law:

Pyramiding and Anxiety Claims
When a mental health condition, such as an anxiety disorder, overlaps with a non-psychiatric condition, VA will avoid “pyramiding.” This means that VA will only compensate for a symptom that a veteran is experiencing once.
If a veteran suffers from an orthopedic condition that causes sleep impairment and a psychiatric condition that also causes sleep impairment, VA will rate that symptom under one of those conditions and not the other. In other words, VA will not compensate a veteran for the same symptom twice.
Hospitalization for Anxiety Disorders
According to VA, periods of hospitalization are considered to be totally disabling. In situations where veterans are hospitalized due to their service-connected anxiety disorders for more than 21 days, they should be entitled to a 100 percent disability rating for the period of their hospitalization.
If veterans are hospitalized for an extended stay of more than six months, they may be assigned a 100 percent total rating not only for the entire length of the hospitalization, but also for an additional six months after the date of discharge. Veterans must tell VA immediately if they are hospitalized to ensure they are compensated properly.
Do Veterans Have To File Separate Claims for Multiple Mental Health Conditions?
No, generally not.
Since mental health conditions share similar symptomatology, VA will consider the combined effects of the conditions to determine the overall level of social and occupational impairment. In other words, even if veterans have another diagnosed mental health condition in addition to their anxiety disorder, VA will usually only assign one disability rating.
When veterans submit a claim for a particular mental health condition, VA will process their claim as a claim for any mental health condition. Therefore, VA does not limit its consideration to the particular mental health condition that was identified in the veteran’s claim.
For example:
- Say a veteran’s initial disability claim is for PTSD, which they submit to VA through the proper channels.
- VA examines the veteran’s case, at which point they determine the evidence of record reflects that the veteran was also diagnosed with depression.
- In this case, VA is required to consider the veteran’s depression in connection with the initial claim for PTSD. As such, the assigned rating will reflect the severity and impact of both mental disorders.
How Much Compensation Can I Earn From an Anxiety Disability Claim?
VA offers multiple benefits to veterans who earn a disability rating for their condition. Some of these benefits include monthly compensation, no-cost healthcare, and educational benefits.
Veterans who have an anxiety rating of 10 percent or higher may qualify for monthly financial compensation at a rate that increases the higher their rating percentage goes.
As of 2026, the VA disability rate benefit amounts are as follows:
- 0 percent disability rating: $0.00 per month
- 10 percent disability rating: $180.42 per month
- 20 percent disability rating: $356.66 per month
- 30 percent disability rating: $552.47 per month
- 40 percent disability rating: $795.84 per month
- 50 percent disability rating: $1,132.90 per month
- 60 percent disability rating: $1,435.02 per month
- 70 percent disability rating: $1,808.45 per month
- 80 percent disability rating: $2,102.15 per month
- 90 percent disability rating: $2,362.30 per month
- 100 percent disability rating: $3,938.58 per month
In addition to these standard rates, eligible veterans with dependents, such as a spouse or children, may qualify for additional compensation, raising the monthly amount they receive.
Special Monthly Compensation for Anxiety
Special Monthly Compensation (SMC) is an additional benefit sometimes awarded to veterans with medical needs that go beyond what VA’s standard financial compensation can offer.
If a veteran’s anxiety is severe enough or combines with another condition to substantially worsen the veteran’s quality of life and ability to care for themselves, then they may be awarded SMC to account for these additional needs. Specifically, this might be the case if a veteran’s anxiety prevents them from taking care of themselves to the point they need regular Aid & Attendance from a professional.
To learn more about the disability benefits available to veterans suffering from anxiety, watch this video breakdown with Alyse Phillips and Jenna Zellmer, attorneys at CCK Law:
Can I Earn Total Disability for Anxiety?
Yes, veterans can earn total disability for anxiety alone, either through a 100 percent schedular disability rating or through Total Disability based on Individual Unemployability (TDIU). TDIU allows a veteran to be compensated at the 100 percent rating even if their schedular rating for anxiety is less than that.
If a veteran’s service-connected anxiety disorder alone, or service-connected anxiety disorder in combination with other service-connected conditions, prevents them from securing and maintaining substantially gainful employment, then they may be entitled to TDIU benefits.
Here, substantially gainful employment typically refers to an annual income that meets or exceeds the federal poverty threshold, though other factors may also influence this determination.
How Do I Appeal a Denied VA Anxiety Claim?
Under the Appeals Modernization Act (AMA), veterans have multiple options to choose from when appealing an unfavorable decision from VA, including the:
- Higher-Level Review Lane
- Supplemental Claim Lane
- Notice of Disagreement Lane (i.e., an appeal to the Board of Veterans’ Appeals).
If veterans are choosing the supplemental claim lane, they must make sure that they are including new and relevant evidence with their claim. “New and relevant” is supposed to be a lower evidentiary standard and can include lay statements, medical evidence, etc. However, it must be something that is relevant to the veteran’s claim that VA has not considered previously.
Overall, AMA is supposed to provide veterans with more choices within the appeals process. Nonetheless, there are still aspects of AMA that remain unclear. As such, veterans are encouraged to consult with Veterans Service Organizations or attorneys when initiating appeals under this new system.
Anxiety Claim Denied by VA? Call CCK Law
If you disagree with a VA decision, consider contacting Chisholm Chisholm & Kilpatrick. An experienced, VA-accredited law firm may offer significant tools and resources in support of your appeal.
While past results do not guarantee future outcomes, CCK Law has had favorable outcomes in 98.5% of its actions before VA and a 95% win rate before the U.S. Court of Appeals for Veterans Claims (federal court). We have recovered over $1 billion in compensation for 36,000+ clients to date.
Contact us online or at 800-544-9144 to tell us about your case.
Frequently Asked Questions
What evidence does VA need for anxiety?
Medical records (private or otherwise) and service records from a veteran’s time in the military are both strong forms of evidence to present to VA for a disability claim for anxiety.
In addition, lay evidence from the veteran or their friends, family, or fellow service members can also be beneficial. Often, veterans do not seek treatment for anxiety due to the stigma associated with mental disorders. Lay evidence, then, can help fill in the gaps if a veteran is missing official service or medical treatment records.
How do I get a 70 percent VA rating for anxiety?
To earn a 70 percent VA disability rating for anxiety, veterans must display that they suffer impairments in most social or occupational areas, like work, school, family relations, judgement, thinking, and mood.
Some symptoms indicative of a 70 percent rating for anxiety include:
- Obsessive rituals interfering with daily activities;
- Near-continuous panic affecting the ability to function independently, appropriately, and effectively;
- Impulse control problems;
- Spatial disorientation;
- Difficulty in adapting to stressful circumstances (including work or work-like settings);
- Neglect of personal appearance or hygiene; and
- Inability to establish and maintain effective relationships.
Importantly, veterans do not need to prove that they suffer all the symptoms listed above; instead, they only need to prove that their personal symptoms are consistent with the severity of some of the above symptoms.
How is anxiety connected to military service?
Military service can be extremely taxing on the body and mind of service members, which can lead to excess worry and anxiety. Some military situations that may prompt the development of an anxiety disorder include:
- Exposure to dangerous or life-threatening situations;
- Chronic stress caused by a culture of hyper-vigilance, strict standards, and harsh punishments;
- Physical exhaustion from lack of sleep or nutrition;
- Separation from friends, family, or a familiar environment;
- Engaging in combat or witnessing traumatic events;
- And more.
Share this Graphic
