VA Disability Ratings for PTSD: A Guide to the PTSD Rating Scale

CCK Law: Our Vital Role in Veterans Law
Veterans living with post-traumatic stress disorder (PTSD) caused by military service are eligible for VA disability compensation. However, it can be challenging to prove PTSD to VA.
The process of demonstrating service connection for PTSD requires unique steps such as establishing a stressor, and the criteria for different PTSD ratings can be vague and unintuitive. Also, PTSD is a significant diagnosis that may make a veteran eligible for special types of VA benefits and compensation, but VA often mistakenly fails to consider these programs when issuing a PTSD rating.
If you disagree with VA’s decision on your initial claim, it is important to remember that you have the right to appeal. There are critical deadlines and other requirements to consider for VA appeals. If you need assistance, consider contacting CCK Law for a free case evaluation.
How VA Assigns Ratings for PTSD
When veterans file a claim for disability benefits for PTSD, VA typically orders a C&P exam to evaluate a veteran’s symptoms and the severity of their condition. During a C&P exam for PTSD, the doctor will determine whether the veteran’s PTSD is “at least as likely as not” related to their military service.
After the C&P exam is complete, VA adjudicators will review it along with all the other evidence in the veteran’s claims file. Once service connection is established for a veteran’s PTSD, VA rates the condition under 38 CFR § 4.130, Diagnostic Code 9411, the Schedule of Ratings for Mental Disorders. VA will also use criteria from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) to assess a PTSD claim.
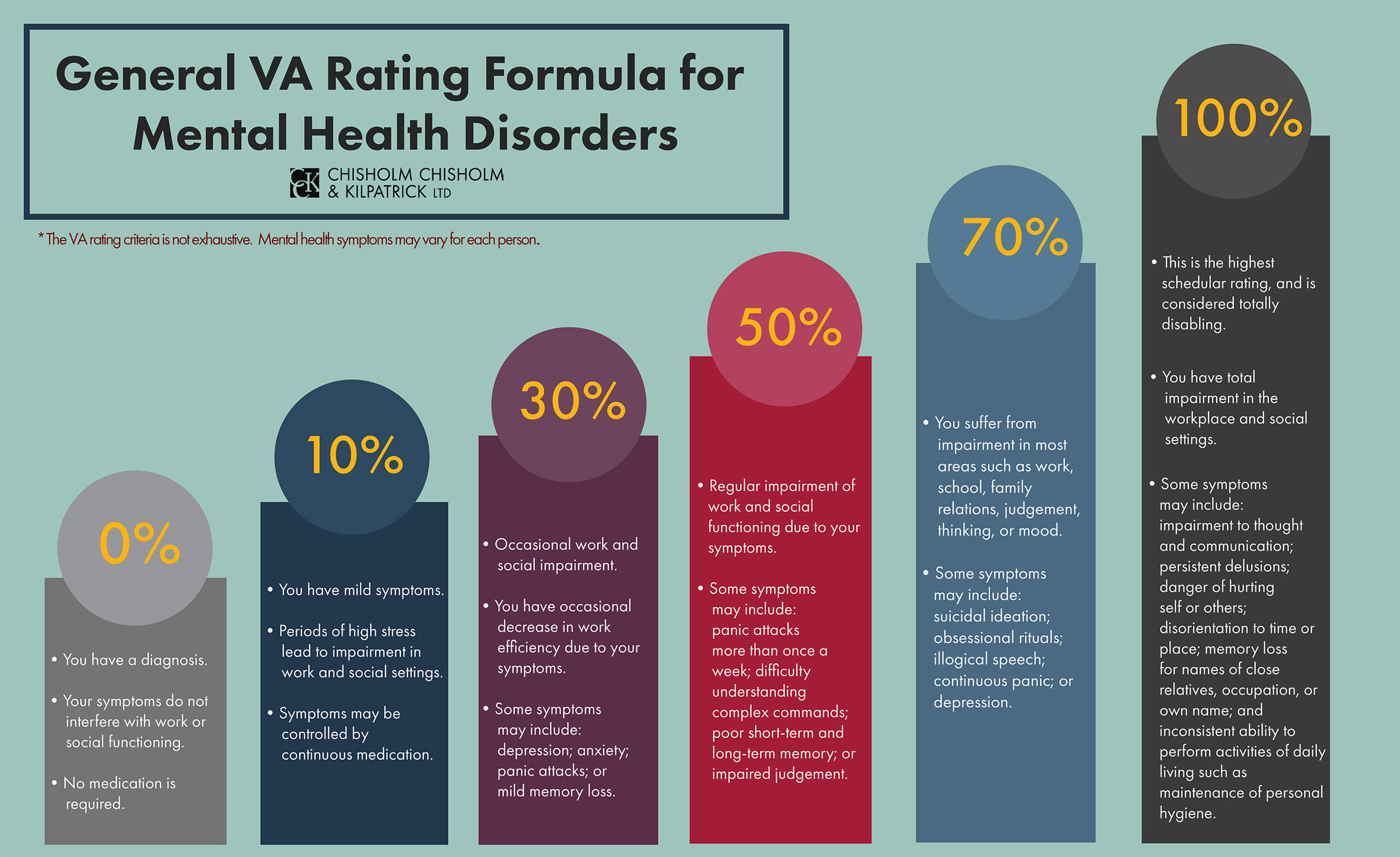
VA then assigns a disability rating of 0, 10, 30, 50, 70, or 100 percent. These ratings are based on the level of social and occupational impairment, as well as the frequency, duration, and severity of symptoms.
0% PTSD Rating
A 0 percent PTSD rating is the lowest possible rating on the PTSD rating scale. This rating will be assigned when:
- “A mental condition has been formally diagnosed, but symptoms are not severe enough either to interfere with occupational and social functioning or to require continuous medication.”
Importantly, 0 percent ratings are noncompensable, meaning the veterans will not receive VA disability compensation for a 0 percent PTSD rating. However, veterans can be eligible for other benefits from VA with a noncompensable rating.

10% PTSD Disability Rating
A 10 percent PTSD rating is the lowest compensable rating offered by VA’s rating criteria for mental disorders. The rating criteria describe very mild or well-controlled symptomology. When assigning a 10 percent PTSD rating, VA will look for the following:
- “Occupational and social impairment due to mild or transient symptoms which decrease work efficiency and ability to perform occupational tasks only during periods of significant stress, or symptoms controlled by continuous medication.”
In this case, a veteran may experience certain PTSD symptoms that are exacerbated during periods of stress but ultimately do not impair their ability to work in most occupations.
The increase in severity of PTSD symptoms during periods of stress implies that the symptoms tend to be episodic. This means that symptoms are not always present and therefore do not significantly interfere with occupational and social functioning. Moreover, even when symptoms are present, it is likely that the veteran can control them with treatment or medication.
30% PTSD Disability Rating
The criteria for a 30 percent rating on the PTSD rating scale are as follows: “Occupational and social impairment with occasional decrease in work efficiency and intermittent periods of inability to perform occupational tasks (although generally functioning satisfactorily, with routine behavior, self-care and conversation normal), due to such symptoms as:
- Depressed mood
- Anxiety
- Suspiciousness
- Panic attacks (weekly or less often)
- Chronic sleep impairment
- Mild memory loss (such as forgetting names, directions, recent events)”
The criteria for a 30 percent PTSD rating describe PTSD symptoms that are beginning to intrude on the veteran’s life despite their best efforts.
For example, “occasional decrease in work efficiency and intermittent periods of inability to perform occupational tasks” might mean that the veteran is starting to periodically miss work due to their lack of motivation associated with PTSD. However, the veteran’s PTSD does not fully prevent them from performing and succeeding in a work environment.
Furthermore, the veteran may experience symptoms such as depressed mood, anxiety, and panic attacks. This may cause them to occasionally isolate themselves but does not completely prohibit them from maintaining relationships with others.
Overall, a 30 percent PTSD rating is assigned when a veteran demonstrates symptoms in a discernable but intermittent manner over time.
50% PTSD Disability Rating
The criteria for a PTSD rating scale for a 50 percent disability rating under 38 CFR § 4.130, Diagnostic Code 9411, are as follows: “Occupational and social impairment with reduced reliability and productivity due to such symptoms as:
- Flattened affect
- Circumstantial, circumlocutory, or stereotyped speech
- Panic attacks more than once a week
- Difficulty in understanding complex commands
- Impairment of short- and long-term memory (e.g., retention of only highly learned material, forgetting to complete tasks)
- Impaired judgment
- Impaired abstract thinking
- Disturbances of motivation and mood
- Difficulty in establishing and maintaining effective work and social relationships.”
The 50 percent PTSD rating criteria involve an escalation in the frequency, duration, and severity of PTSD symptoms. The rating also considers several additional symptoms. If a veteran receives a 50 percent PTSD rating, they are likely beginning to display cognitive deficits such as difficulty following instructions, or they are making decisions that depart from past behavior.
Some of the mood-associated symptomology may also begin to manifest in physiological ways like flattened affect. For example, symptoms like depression and anxiety are causing the veteran to speak in a monotone and lack facial expressions.
The overall level of occupational and social impairment is also higher in a veteran assigned a 50 percent PTSD rating. The symptoms mentioned above cause a decrease in the veteran’s ability to efficiently complete work-related tasks.
70% PTSD Disability Rating
A 70 percent PTSD disability rating is one step below the highest schedular rating for the condition. The key reason for most 70 percent PTSD ratings is that symptoms are causing significant levels of impairment, both occupationally and socially.
This rating is typically assigned to veterans with PTSD symptoms that are one step below totally disabling. The criteria for a 70 percent rating on the PTSD rating scale are as follows:
“Occupational and social impairment, with deficiencies in most areas, such as work, school, family relations, judgment, thinking, or mood, due to such symptoms as:
- Suicidal ideation
- Obsessional rituals which interfere with routine activities
- Speech intermittently illogical, obscure, or irrelevant
- Near-continuous panic or depression affecting the ability to function independently, appropriately, and effectively
- Impaired impulse control (such as unprovoked irritability with periods of violence)
- Spatial disorientation
- Neglect of personal appearance and hygiene
- Difficulty in adapting to stressful circumstances (including work or a work-like setting)
- Inability to establish and maintain effective relationships.”
Notably, the 70 percent disability rating criteria for PTSD includes the widest array of symptoms of all rating levels. A veteran who receives a 70 percent PTSD rating usually suffers from all the symptoms included in lower ratings and at a higher frequency, severity, and duration. The veteran is almost always in a state of panic or depression that interferes with their ability to interact with others.
The veteran may also have trouble controlling their emotions in a way that leads to violent outbursts or conflict with others. The level of occupational and social impairment here is evidenced by the veteran’s inability to hold down a job or complete classes for school.
The veteran may engage in obsessive rituals such as checking the locks on their doors multiple times throughout the course of a day as a result of being hypervigilant.
100% PTSD Disability Rating
A 100 percent PTSD rating is often difficult to obtain from VA because it requires a veteran’s symptoms to be so severe that they are totally impaired and unable to function in everyday life.
While the symptoms listed in the 70 percent rating criteria involve a high level of impairment, the jump to 100 percent is even more significant. The criteria for a 100 percent PTSD rating are as follows: “Total occupational and social impairment, due to such symptoms as:
- Gross impairment in thought processes or communications
- Persistent delusions or hallucinations
- Grossly inappropriate behavior
- Persistent danger of hurting self or others
- Intermittent inability to perform activities of daily living (including maintenance of minimal personal hygiene)
- Disorientation to time or place
- Memory loss for names of close relatives, own occupation, or own name.”
The abovementioned symptoms represent a substantial decline in cognitive and emotional functioning as compared to the rating criteria for lower percentages. Importantly, this decline results in a total impairment when it comes to a veteran’s work life and personal life.
Specifically, a veteran may experience hearing voices or perceiving things that are not actually present. Self-injurious behaviors and suicide attempts are also consistent with a 100 percent rating.
In addition to suicidality, a 100 percent on the PTSD rating scale can also include homicidal ideation, which means a veteran might have thoughts of harming others.
An “intermittent inability to perform activities of daily living” may be seen by a veteran feeling too depressed to get out of bed, take a shower, or change clothes. All these symptoms and behaviors are consistent with the highest level of impairment as reflected by the rating scale.
Frequently Asked Questions About PTSD Ratings
Do veterans need to have all of the symptoms listed to receive a PTSD rating?
No. In the case of Mauerhan v. Principi, the Court of Appeals for Veterans Claims (CAVC) established that the symptoms listed in Diagnostic Code 9411 (PTSD) are not intended to constitute an exhaustive list, but rather serve as examples of the type and degree of symptoms, or their effects, that would justify a particular rating.
In other words, while the General Rating Formula for Mental Disorders describes multiple symptoms for each disability rating, a veteran does not need to exhibit every symptom named on the PTSD rating scale to qualify for a specific rating.
For example, a veteran who only experiences suicidal ideation and near-continuous panic or depression might still receive at 70 percent PTSD disability rating.
What if a veteran’s symptoms are consistent with more than one PTSD rating?
Since PTSD is a complex condition and many of the symptoms within the rating criteria overlap, a veteran may not fall clearly into one percentage category.
For example, a veteran may experience mild memory loss in addition to impaired judgment and flattened affect, meaning they have symptoms listed under both the 30 percent and 50 percent rating descriptions on the PTSD rating scale.
Since it is not possible to split the difference between the two ratings, VA must choose one to award. According to 38 CFR § 4.7, the higher evaluation should be assigned if the disability “more clearly meets the criteria required for that rating.” Basically, having symptoms from a lower rating should not interfere with a veteran’s ability to get a higher rating.
It is important to note that veterans do not need to meet all of the criteria listed in VA’s rating schedule to qualify for that particular rating.
Is PTSD an automatic 50% rating?
No. Many veterans have been led to believe that successful PTSD claims always receive an automatic 50% PTSD rating. This is not entirely accurate. The automatic 50 percent rating only applies under specific circumstances.
According to 38 CFR § 4.129, “when a mental disorder that develops in service as a result of a highly stressful event is severe enough to bring about the veteran’s release from active military service, the rating agency shall assign an evaluation of not less than 50 percent and schedule an examination within the six month period following the veteran’s discharge to determine whether a change in evaluation is warranted.”
In other words, an automatic 50 percent rating will only be granted to veterans if their PTSD caused them to be discharged from military service, and this automatic 50 percent disability rating will only last for six months following the veteran’s separation from service.
After six months have passed, VA will conduct a new PTSD evaluation to determine the veteran’s current condition. While it is possible that the veteran will again be assigned a 50 percent rating for their PTSD, it is also possible that the rating will be changed.
What is the most common VA disability rating for PTSD?
Currently, many veterans who receive VA disability for their service-connected PTSD are rated at the 70 percent level. A 70 percent PTSD rating reflects impairment in most areas of life, including work, school, family relations, judgment, thinking, and mood.
These effects are often more easily documented than symptoms from other ratings. This PTSD rating also offers more examples of symptoms that affect occupational and social function, which can further improve the odds of demonstrating a disability.
Note that a veteran with a 70 percent disability rating for PTSD may be struggling to find or maintain employment. In such cases, it may be beneficial for the veteran to file a claim for total disability based on individual unemployability.
Can I get TDIU for PTSD?
If a veteran’s PTSD significantly impairs their ability to work, they may be eligible for a rating of Total Disability based on Individual Unemployability (TDIU) — a VA benefit that allows veterans to receive compensation at the 100 percent rate if their service-connected condition(s) prevent them from securing and maintaining substantially gainful employment.
There are two ways veterans can qualify for TDIU based on their PTSD under VA’s regulation 38 CFR § 4.16: Schedular and Extraschedular.
A veteran may be eligible for schedular TDIU for their PTSD under either of the following conditions:
- The veteran’s PTSD must be rated at 60 percent or higher on its own; or
- The veteran must have a combined rating of 70 percent or higher when the PTSD is taken together with other service-connected conditions and at least one of those conditions is rated at 40 percent or higher on its own.
Even if a veteran does not meet the eligibility requirements listed above, they may still qualify for TDIU on an extraschedular basis. Extraschedular TDIU exists for veterans who are unable to “secure and follow substantially gainful employment” due to service-connected conditions, but who fail to meet the rating percentages for schedular TDIU described above.
In these circumstances, VA refers the veteran’s claim for TDIU to the Director of Compensation Service for extraschedular consideration. The Director will then review factors such as the veteran’s unique conditions, employment history, and educational and vocational progress before making a decision about whether to grant TDIU status.
How much is the VA disability compensation for PTSD?
Each disability rating on VA’s rating schedule grants a different monthly benefit amount. The higher the disability rating, the more a veteran receives in monthly compensation.
As of 2026, the VA disability rate benefit amounts are as follows:
- 0 percent disability rating: $0.00 per month
- 10 percent disability rating: $180.42 per month
- 20 percent disability rating: $356.66 per month
- 30 percent disability rating: $552.47 per month
- 40 percent disability rating: $795.84 per month
- 50 percent disability rating: $1,132.90 per month
- 60 percent disability rating: $1,435.02 per month
- 70 percent disability rating: $1,808.45 per month
- 80 percent disability rating: $2,102.15 per month
- 90 percent disability rating: $2,362.30 per month
- 100 percent disability rating: $3,938.58 per month
Veterans with conditions rated at least 30 percent disabling can qualify to receive additional benefits for dependents in their household, such as a spouse, child, or dependent parent. Even if a veteran already has a 100 percent disability rating and thus receives maximum compensation, they can receive additional compensation for dependents.
Need Help With Your PTSD VA Disability Appeal?
If you received a denial or insufficient rating for your PTSD, you should consider a prompt appeal. The appeals process can be lengthy and difficult. The accredited VA disability attorneys and advocates at Chisholm Chisholm & Kilpatrick LTD may be able to assist you.
The case evaluation is free, so call our office today at 800-544-9144 or contact us online to request your free evaluation.