Most Common Back Conditions Veterans Experience & Their Ratings

CCK Law: Our Vital Role in Veterans Law
Back injuries are one of the most common types of injuries servicemembers experience, due to the intense physicality associated with military service. Back injuries can occur during training or combat. They can occur by vehicle accidents, falls, carrying heavy gear, or even with other common duties.
As with most medical conditions, VA disability ratings for back pain depend on a variety of factors and can vary significantly.
How Does VA Rate Back Conditions?
VA rates most back conditions under 38 CFR § 4.71a, Schedule of Ratings, Musculoskeletal System, General Rating Formula for Diseases and Injuries of the Spine. The criteria are based largely on a veteran’s range of motion.
Different diagnostic codes within this formula are used to rate different back disabilities. The ratings issued can range from 0 to 100 percent.
Generally, veterans will need to attend a C&P exam to measure how far they can bend forwards, backwards, and side to side, using a goniometer.
VA will then determine the severity of back condition based on the range of motion measurements. When issuing a rating, VA must also take into account functional loss (pain during motion) and flare-ups.
Common Back Conditions
#1. Lumbosacral and Cervical Strain
Lumbosacral or cervical strain is an injury of the ligaments, tendons and/or muscles of the low back or neck, respectively. The injury usually results from stretching that causes a small tear in these tissues.
Lumbosacral and cervical strain are typically caused by overuse and trauma. Pain is a very common symptom of lumbosacral and cervical strain, as well as trouble bending or having limited range of motion.
VA rates lumbosacral and cervical strain under Diagnostic Code 5237.
Ratings for Lumbosacral and Cervical Strain
- 100% – unfavorable ankylosis of the entire spine
- 50% – unfavorable ankylosis of the entire thoracolumbar spine
- 40% – unfavorable ankylosis of the entire cervical spine; or, forward flexion of the thoracolumbar spine 30 degrees or less; or, favorable ankylosis of the entire thoracolumbar spine
- 30% – forward flexion of the cervical spine 15 degrees or less; or, favorable ankylosis of the entire cervical spine
- 20% – forward flexion of the thoracolumbar spine greater than 30 degrees but not greater than 60 degrees; or, forward flexion of the cervical spine greater than 15 degrees but not greater than 30 degrees; or, the combined range of motion of the thoracolumbar spine not greater than 120 degrees; or, the combined range of motion of the cervical spine not greater than 170 degrees; or, muscle spasm or guarding severe enough to result in an abnormal gait or abnormal spinal contour such as scoliosis, reversed lordosis, or abnormal kyphosis
- 10% – forward flexion of the thoracolumbar spine greater than 60 degrees but not greater than 85 degrees; or, forward flexion of the cervical spine greater than 30 degrees but not greater than 40 degrees; or, combined range of motion of the thoracolumbar spine greater than 120 degrees but not greater than 235 degrees; or, combined range of motion of the cervical spine greater than 170 degrees but not greater than 335 degrees; or, muscle spasm, guarding, or localized tenderness not resulting in abnormal gait or abnormal spinal contour; or, vertebral body fracture with loss of 50 percent or more of the height
#2. Degenerative Disc Disease
Degenerative Disc Disease (DDD) usually occurs in the lower back or neck. DDD is a condition where the discs between vertebrae lose cushioning, fragment, and herniate.
Pain can frequently occur with degenerative disc disease, although not in every case. In some situations, DDD can result in numbness and tingling in the upper or lower extremities.
VA also rates degenerative disc disease based on range of motion testing (DC 5242).
Ratings for Degenerative Disc Disease
VA rates degenerative disc disease under 38 CFR § 4.71a, Schedule of Ratings – Musculoskeletal System, Diagnostic Code 5242. The rating criteria for this diagnostic code is virtually the same as Diagnostic Code 5003, which is used to rate degenerative arthritis.
If degenerative arthritis is established by X-ray findings, the veteran’s condition will be rated based on limitation of motion under the appropriate diagnostic codes for the specific joint or joints involved. However, if the limitation of motion of the specific joint or joints involved is noncompensable under the appropriate diagnostic codes, a rating of 10 percent will be applied for each major joint or group of minor joints affected by limitation of motion. Finally, in the absence of limitation of motion, a veteran’s degenerative disc disease will be rated as follows:
- 10% – with X-ray evidence of involvement of 2 or more major joints or 2 or more minor joint groups, with occasional incapacitating exacerbations
- 20% –with X-ray evidence of involvement of 2 or more major joints or 2 or more minor joint groups
When assigning a disability rating based on the severity of symptoms, VA must take into account both anatomical damage and functional loss. Importantly, limitation of motion must be objectively confirmed by findings such as swelling, muscle spasms, or satisfactory evidence of painful motion.
#3. Intervertebral Disc Syndrome
Intervertebral Disc Syndrome (IVDS), also known as a bulging or herniated disc, is a back condition that involves the irritation of the nerve root and causes sharp, chronic pain. Additional symptoms of IVDS can include numbness or tingling in the lower extremities, and weakness. VA currently rates IVDS under Diagnostic Code 5243, and each rating is based on how frequently, and for how long, a veteran is prescribed bed rest for their IVDS.
At present, physicians generally agree that the practice of prescribing bed rest for IVDS can actually be harmful for a veteran’s recovery. Bed rest can lead to stiffening of the joints and can weaken the muscles. As a result, physicians generally do not prescribe bed rest for IVDS. Instead, physical therapy and medication for pain are considered more effective treatments.
Ratings for Intervertebral Disc Disease
- 60% – with incapacitating episodes having a total duration of at least 6 weeks during the past 12 months
- 40% – with incapacitating episodes having a total duration of at least 4 weeks but less than 6 weeks during the past 12 months
- 20% –with incapacitating episodes having a total duration of at least 2 weeks but less than 4 weeks during the past 12 months
- 10% –with incapacitating episodes having a total duration of at least one week but less than 2 weeks during the past 12 months”
#4. Sciatic Nerve Issues
Sciatic nerve conditions involve pain that radiates along the path of the sciatic nerve, traveling from the lower back down through the legs. It most often occurs when the sciatic nerve is compressed or pinched, usually by a herniated disk in the spine or an overgrowth of bone on the vertebrae.
Other symptoms include numbness, tingling, burning sensation, and muscle weakness.
While a nerve issue and symptoms of sciatic nerve issues often affect the lower extremities, the issue technically begins in the back.
Veterans can be rated under three different diagnostic codes for sciatic nerve issues depending on their symptoms and severity.
Ratings for Sciatic Nerve Issues
DC 8520 – Paralysis of the Sciatic Nerve
- 80% – complete paralysis in which all the muscles of the leg below the knee fail to work, causing serious difficulty in bending the knee
- 60% – incomplete but severe paralysis marked by muscular atrophy, poor blood circulation, and limited functionality of the affected body part
- 40% – incomplete but moderately severe paralysis
- 20% – incomplete but moderate paralysis
- 10% – incomplete but mild paralysis
DC 8620—Neuritis of the Sciatic Nerve
- 60% – severe neuritis marked by a loss of reflexes, loss of sensation, and muscle atrophy; seriously limited functionality of the affected body part
- 40% – moderately severe neuritis
- 20% – moderate neuritis
- 10% – mild neuritis
DC 8720—Neuralgia of the Sciatic Nerve
- 20% – moderate neuralgia involving tingling, numbness, and moderate to severe pain, along with interference with the affected limb’s functionality
- 10% – mild neuralgia causing tingling or mild pain, with only minor interference with the limb’s functionality
Importantly, there is no disability rating for severe neuralgia.
Secondary Conditions to Back Disabilities
Oftentimes, back disabilities can cause or aggravate a variety of other conditions.
Examples include:
- Radiculopathy – can get a second rating
- Gastrointestinal or stomach issues
- Hip/leg/foot disabilities
- Effects of medication
- Effects of obesity caused by lack of ability to exercise due to a back problem
- Depression

Veterans may be able to receive secondary service connection for any condition(s) caused by or related to their back disability. To establish secondary service connection for a condition caused or aggravated by a back condition, veterans will need to submit:
- A current diagnosis of the secondary injury, illness, or disability; and
- Medical evidence showing a link between your service-connected back disability and the secondary condition.
To file a claim for secondary service connection, veterans will follow much of the same process they did for establishing service connection for their back disability. Veterans can fill out and submit VA Form 21-526EZ. Veterans may do so online at VA.gov, in person at their local VA Regional Office, or with help from an accredited veterans’ advocate or attorney.
TDIU With Common Back Disabilities
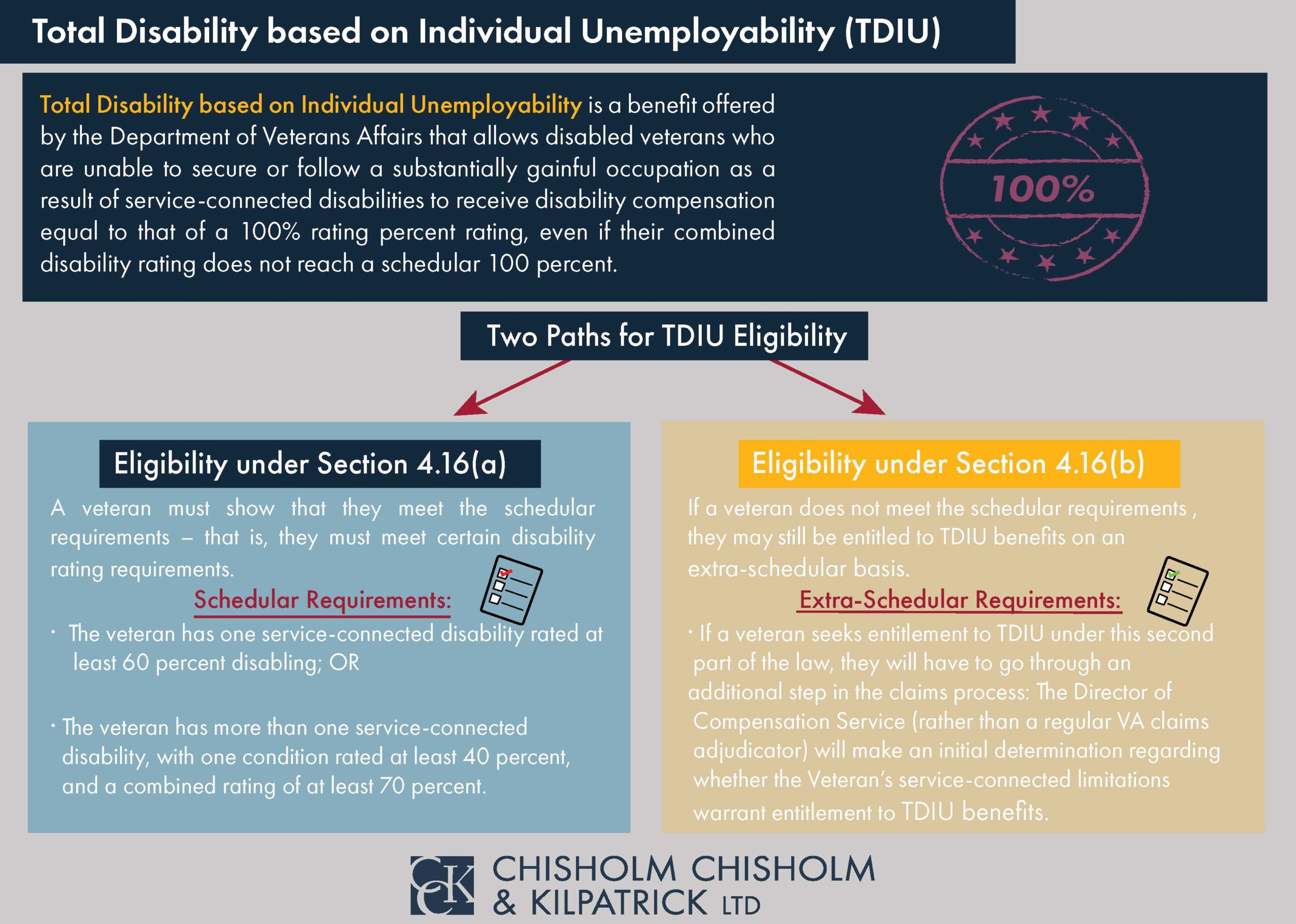
Total disability based on individual unemployability (TDIU) is a monthly benefit that compensates veterans who are unable to gain or maintain substantial employment because of their service-connected disabilities. TDIU pays veterans at the 100 percent rating level, even if their combined rating does not equal 100 percent.
VA outlines TDIU regulations under 38 CFR § 4.16, which includes subsections (a) and (b). In order to qualify for TDIU under 38 CFR § 4.16(a), or schedular TDIU, a veteran must have:
- One service-connected condition rated at 60% or higher; or
- Two or more service-connected conditions, one of which is rated at 40% or higher, with a combined rating of 70% or higher.
Notably, both ratings for a back condition and a secondary condition can contribute to the veteran’s overall combined rating. For example, a veteran may be eligible for schedular TDIU if they receive a 60 percent rating for Intervertebral Disc Disease and a 10 percent rating for depression. Veterans who do not meet the schedular requirements under 38 CFR § 4.16(a) may still be considered for extraschedular TDIU under § 4.16(b).
Was Your Disability Benefits Claim for a Back Condition Denied?
The experienced veterans’ advocates at Chisholm Chisholm & Kilpatrick LTD have helped many veterans win VA disability benefits for back conditions, and may be able to help you do the same. If your VA disability claim for a back condition was denied, contact our office for a free case evaluation.
Share this Graphic
