Getting Veterans (VA) Disability for Hypertension
CCK Law: Our Vital Role in Veterans Law
If you served in the military and developed hypertension (high blood pressure) as a result of service, you could be eligible for disability benefits from the U.S. Department of Veteran Affairs. To receive a grant of veterans (VA) disability for hypertension, you must establish that it resulted from an in-service event, injury, or illness.
Even with a valid claim, the application process for VA disability can be complex and unpredictable, and many veterans receive denials despite meeting the necessary criteria. The VA-accredited advocates and attorneys at Chisholm Chisholm & Kilpatrick may be able to help.
We have argued many of the most influential cases in veterans law and recovered over $1 billion in compensation for over 30,000 veterans or dependents. (Past results do not guarantee future outcomes.) Let us put our experience to work for you. Contact us online or at 800-544-9144 to tell us about your case.
How Can a Veteran Prove to VA That Their Hypertension Is Service Connected?
- VA will presume service connection for hypertension if you received a diagnosis during active duty or up to one year after your release.
- VA will also presume service connection if you served at times and places where you might have been exposed to Agent Orange. See the section called “Presumptive Service Connection for Hypertension after Agent Orange Exposure” below.
- If you received your hypertension diagnosis more than a year after service and were not exposed to Agent Orange, then you must prove “direct” service connection, which has three steps.
Step 1 (Direct Service Connection): Current Diagnosis of Hypertension
Normal blood pressure is defined as a reading below 120/80 mmHg (millimeters of mercury). This means the systolic (top) number is less than 120 and the diastolic (bottom) number is less than 80. To be eligible for monthly compensation, your blood pressure must have a systolic measurement (the top number) of 160 or more and a diastolic measurement (the bottom number) of 100 or more.
Step 2: In-Service Cause for Hypertension
For direct service connection, veterans must provide evidence of an in-service event, injury, or illness that occurred during military service and caused their hypertension. Evidence such as a medical opinion can be very helpful.
Step 3: Nexus (Medical Opinion)
The final requirement for direct service connection is a nexus, which is generally a medical opinion stating that your current hypertension (Step 1) was caused by your in-service event, injury, or illness (Step 2).
Note that VA may also order a compensation and pension (C&P) exam in order to establish service connection. A C&P exam is generally run by a medical professional employed or contracted by VA, and will help VA determine the severity of a veteran’s hypertension, as well as its possible service connection.
Presumptive Service Connection for Hypertension Due to Agent Orange Exposure
Agent Orange is an herbicide that was used extensively throughout the Vietnam War Era. Medical evidence has linked hypertension to Agent Orange exposure. Therefore, the Honoring Our PACT Act extended presumptive service connection to veterans who developed hypertension as a result of Agent Orange exposure.
In other words, veterans who served in places and at times where they might have been exposed to Agent Orange, then develop hypertension at any point, will be assumed by VA to have service connection.
In order to be eligible for this presumption, the veteran needs to have served in one of the following:
- The Republic of Vietnam between January 9, 1962, and May 7, 1975;
- Thailand, at any US or Thai base, January 9, 1962, and June 30, 1976;
- Laos between December 1, 1965 an September 30, 1969;
- Cambodia, specifically at Mimot or Krek, Kampong Cham Province, between April 1969 and April 30, 1969;
- Guam or American Samoa or in the territorial waters thereof between January 9, 1962, and July 30, 1980;
- Johnston Atoll island or Johnston Atoll the ship between January 1, 1972, and September 30, 1977
If the veteran has a diagnosis of hypertension and served an above-listed location and time period, they should be eligible for presumptive service connection.

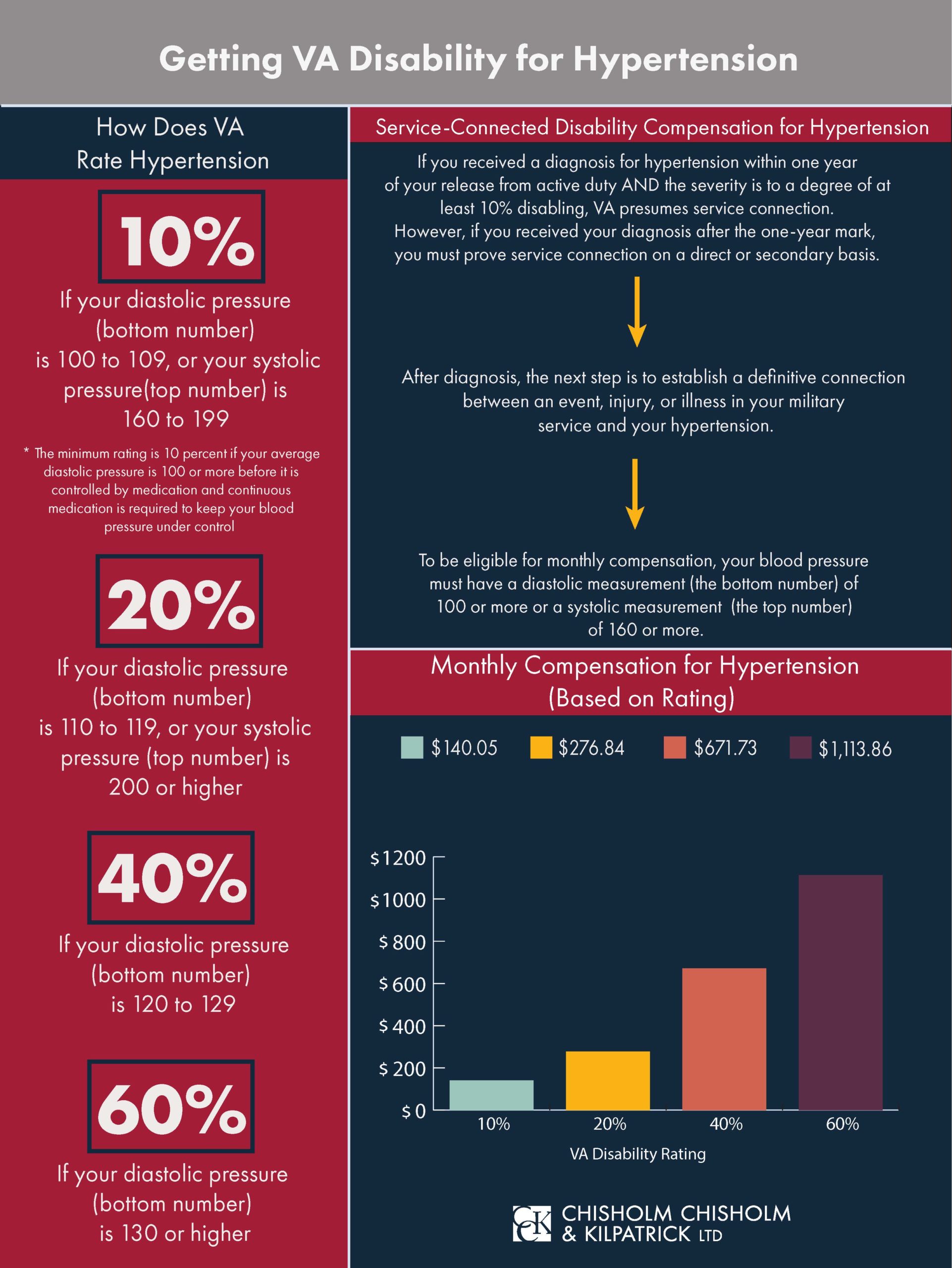
How Does VA Rate Hypertension?
The amount of your monthly compensation for hypertension depends on your disability rating. VA assigns this rating based on the severity of your condition.
If you are granted service connection, you will receive a rating from 0 to 100 percent (in 10-percent increments). Your hypertension must be rated at 10 percent or higher to receive monthly compensation (although a 0 percent rating still qualifies you for health care and other ancillary benefits).
Your rating depends on your blood pressure reading. Per § 4.104-10 Diagnostic Code 7101:
- If your diastolic pressure (bottom number) is 130 or higher: 60 percent rating
- If your diastolic pressure is 120 to 129: 40 percent rating
- If your diastolic pressure is 110 to 119, or your systolic pressure (top number) is 200 or higher: 20 percent rating
- If your diastolic pressure is 100 to 109, or your systolic pressure is 160 to 199: 10 percent rating
Your diagnosis of hypertension must be supported by evidence proving that two or more blood pressure readings were performed on three different days. This rule is in place to ensure that a diagnosis of hypertension is not based solely on “readings taken on a single, perhaps unrepresentative, day.”
If you undergo consecutive sets of blood pressure readings in the same month, VA gives veterans the “benefit of the doubt” and assigns them the highest rating based on those test results. If two sets of readings are taken months apart while a veteran’s claim is being decided, the veteran is assigned the rating that correlates to the first set of blood pressure levels.
If the second set of blood tests yields higher blood pressure levels, a staged rating is assigned effective from the date of the second set of tests.
What Is the VA Monthly Compensation for Hypertension?
Veterans with hypertension can be assigned ratings ranging from 0 percent to 60 percent.
As of 2026, the VA disability rate benefit amounts are as follows:
- 0 percent disability rating: $0.00 per month
- 10 percent disability rating: $180.42 per month
- 20 percent disability rating: $356.66 per month
- 40 percent disability rating: $795.84 per month
- 60 percent disability rating: $1,435.02 per month
If VA rates your hypertension at 30 percent or higher, you may be able to receive additional benefits on behalf of qualified dependents living in your home. Usually, this means a spouse, children, or parents who live in your household and depend on you financially.
Chisholm Chisholm & Kilpatrick Can Help You Pursue Benefits
We hope this blog helped answer your questions.
Need personalized assistance? If VA has made any kind of decision related to your claim, then CCK Law may be able to help. Contact us online or at 800-544-9144 for a free case evaluation.
(As of 2026, federal law prohibits agents and attorneys from charging veterans a fee to file an initial VA claim. In these cases, you will need to find a VA-accredited representative or VSO to assist you.)
Looking for more information? CCK Law hosts over 2,500 pages and 1,100 videos of free veterans law content. Search our blog or browse our YouTube channel for guides, explainers, and updates on VA benefits topics.
Stay current. Veterans disability law and VA policy change frequently. Follow CCK Law on social media using the links at the bottom of this page, or subscribe to one of our newsletters for updates tailored to your situation.
Share this Graphic